
| [1] |
Gregg E W, Li Y, Wang J, et al. Changes in diabetes-related complications in the United States, 1990–2010. The New England Journal of Medicine, 2014, 370 (16): 1514–1523. doi: 10.1056/NEJMoa1310799
|
| [2] |
King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. British Journal of Clinical Pharmacology, 1999, 48 (5): 643–648. doi: 10.1046/j.1365-2125.1999.00092.x
|
| [3] |
Sharma U, Pal D, Prasad R. Alkaline phosphatase: an overview. Indian Journal of Clinical Biochemistry, 2014, 29 (3): 269–278. doi: 10.1007/s12291-013-0408-y
|
| [4] |
Sabarudin A, Sakti S P, Aulanni’am, et al. Recent advances in nephropathy biomarker detections using paper-based analytical devices. Analytical Sciences, 2022, 38 (1): 39–54. doi: 10.2116/analsci.21SAR10
|
| [5] |
van Hoeven K H, Factor S M. The diabetic heart: clinical, experimental and pathological features. Acta Cardiologica, 1991, 46 (3): 329–339.
|
| [6] |
Wang J, Shu Y Q. Research progress in the pathogenesis of type 2 diabetic osteoporosis. Clinical Journal of Traditional Chinese Medicine, 2012, 24 (2): 183–184. (in Chinese) doi: 10.16448/j.cjtcm.2012.02.037
|
| [7] |
Sheu A, Greenfield J R, White C P, et al. Assessment and treatment of osteoporosis and fractures in type 2 diabetes. Trends in Endocrinology & Metabolism, 2022, 33 (5): 333–344. doi: 10.1016/j.tem.2022.02.006
|
| [8] |
Cai G Y, Ge X L, Wei L, et al. Observation of level of bone gla protein in serum. Chinese Journal of Osteoporosis, 1999, 5 (2): 29–32.(in Chinese)
|
| [9] |
Takashi Y, Kawanami D. The role of bone-derived hormones in glucose metabolism, diabetic kidney disease, and cardiovascular disorders. International Journal of Molecular Sciences, 2022, 23 (4): 2376. doi: 10.3390/ijms23042376
|
| [10] |
Krege J H, Lane N E, Harris J M, et al. PINP as a biological response marker during teriparatide treatment for osteoporosis. Osteoporosis International, 2014, 25 (9): 2159–2171. doi: 10.1007/s00198-014-2646-0
|
| [11] |
Delmas P D. Biochemical markers of bone turnover in Paget’s disease of bone. Journal of Bone and Mineral Research, 1999, 14: 66–69. doi: 10.1002/jbmr.5650140213
|
| [12] |
Mei C L, Wang N. Modern Regression Analysis Method (Chinese Edition). Beijing: Science Press, 2012 .
|
| [13] |
Wang J, Wang F, Liu Y, et al. Multiple linear regression and artificial neural network to predict blood glucose in overweight patients. Experimental and Clinical Endocrinology & Diabetes, 2016, 124 (1): 34–38. doi: 10.1055/s-0035-1565175
|
| [14] |
García-Martín A, Reyes-García R, García-Castro J M, et al. Role of serum FSH measurement on bone resorption in postmenopausal women. Endocrine, 2012, 41: 302–308. doi: 10.1007/s12020-011-9541-7
|
| [15] |
Cabrera C D, Henríquez M S, Traba M L, et al. Biochemical markers of bone formation in the study of postmenopausal osteoporosis. Osteoporosis International, 1998, 8 (2): 147–151. doi: 10.1007/BF02672511
|
| [16] |
Shan P F, Wu X P, Zhang H, et al. Bone mineral density and its relationship with body mass index in postmenopausal women with type 2 diabetes mellitus in mainland China. Journal of Bone and Mineral Metabolism, 2009, 27 (2): 190–197. doi: 10.1007/s00774-008-0023-9
|
| [17] |
Im J A, Yu B P, Jeon J Y, et al. Relationship between osteocalcin and glucose metabolism in postmenopausal women. Clinica Chimica Acta, 2008, 396 (1/2): 66–69. doi: 10.1016/j.cca.2008.07.001
|
| [18] |
Wei J, Karsenty G. An overview of the metabolic functions of osteocalcin. Current Osteoporosis Reports, 2015, 13 (3): 180–185. doi: 10.1007/s11914-015-0267-y
|
| [19] |
Rossini M, Gatti D, Zamberlan N, et al. Long-term effects of a treatment course with oral alendronate of postmenopausal osteoporosis. Journal of Bone and Mineral Research, 1994, 9 (11): 1833–1837. doi: 10.1002/jbmr.5650091121
|
| [20] |
Conte C, Epstein S, Napoli N. Insulin resistance and bone: a biological partnership. Acta Diabetologica, 2018, 55 (4): 305–314. doi: 10.1007/s00592-018-1101-7
|
| [21] |
Masaki H, Miki T. Bone and calcium metabolism in elderly women. Clinical Calcium, 2011, 21 (9): 1361–1367.
|
| [22] |
Keizman D, Ish-Shalom M, Berliner S, et al. Low uric acid levels in serum of patients with ALS: further evidence for oxidative stress? Journal of the Neurological Sciences, 2009, 285 (1/2): 95–99. doi: 10.1016/j.jns.2009.06.002
|
| [23] |
Ahn S H, Lee S H, Kim B J, et al. Higher serum uric acid is associated with higher bone mass, lower bone turnover, and lower prevalence of vertebral fracture in healthy postmenopausal women. Osteoporosis International, 2013, 24 (12): 2961–2970. doi: 10.1007/s00198-013-2377-7
|
| [24] |
Cui R, Zhou L, Li Z, et al. Assessment risk of osteoporosis in Chinese people: relationship among body mass index, serum lipid profiles, blood glucose, and bone mineral density. Clinical Interventions in Aging, 2016, 11: 887–895. doi: 10.2147/CIA.S103845
|
| [25] |
Ha J, Jo K, Lim D J, et al. Parathyroid hormone and vitamin D are associated with the risk of metabolic obesity in a middle-aged and older Korean population with preserved renal function: A cross-sectional study. PLoS ONE, 2017, 12 (4): e0175132. doi: 10.1371/journal.pone.0175132
|
| [26] |
Tintut Y, Parhami F, Tsingotjidou A, et al. 8-Isoprostaglandin E2 enhances receptor-activated NFκB ligand (RANKL)-dependent osteoclastic potential of marrow hematopoietic precursors via the cAMP pathway. The Journal of Biological Chemistry, 2002, 277 (16): 14221–14226. doi: 10.1074/jbc.M111551200
|
| [27] |
Go J H, Song Y M, Park J H, et al. Association between serum cholesterol level and bone mineral density at lumbar spine and femur neck in postmenopausal Korean women. Korean Journal of Family Medicine, 2012, 33 (3): 166–173. doi: 10.4082/kjfm.2012.33.3.166
|
| [28] |
He L, Huang L. Correlation between hypertension and primary osteoporosis. Modern Chinese Clinical Medicine, 2008, 15 (2): 1–3. (in Chinese)
|
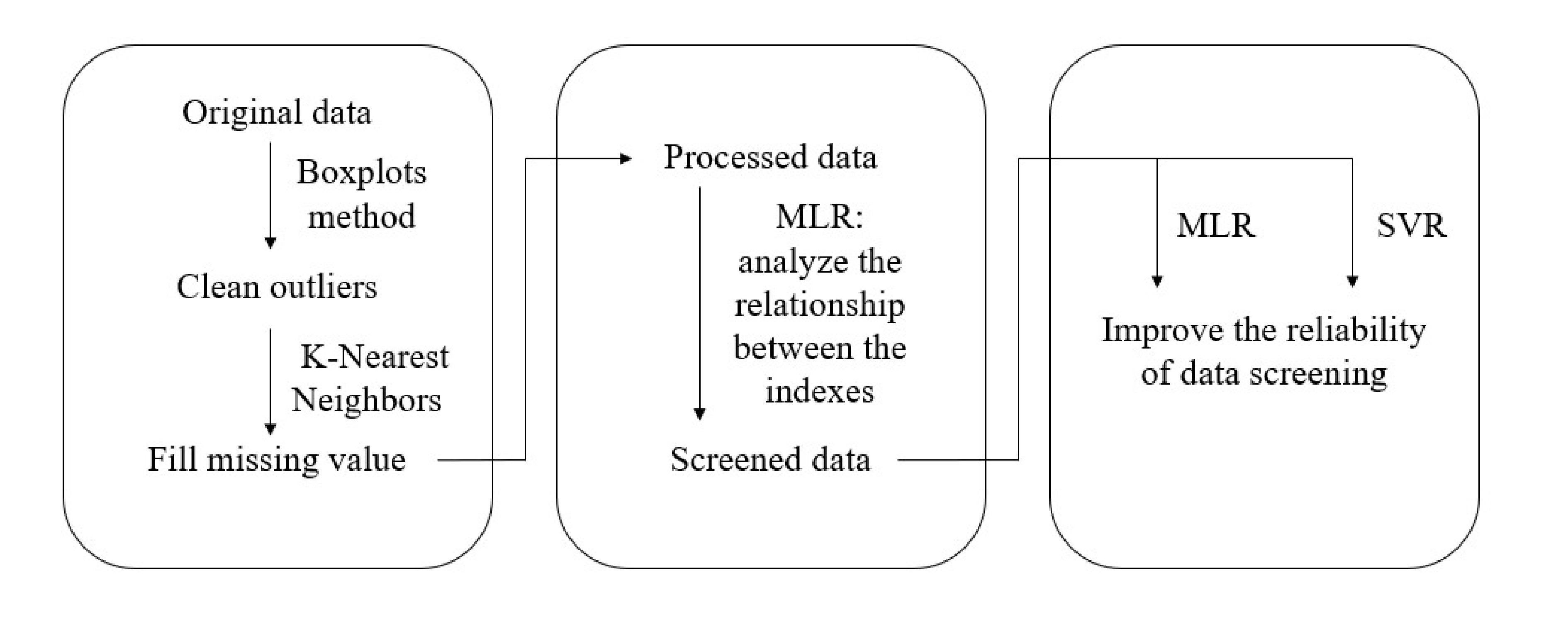
Figure 1. The pipeline of MLR and SVR models for clinical datasets.
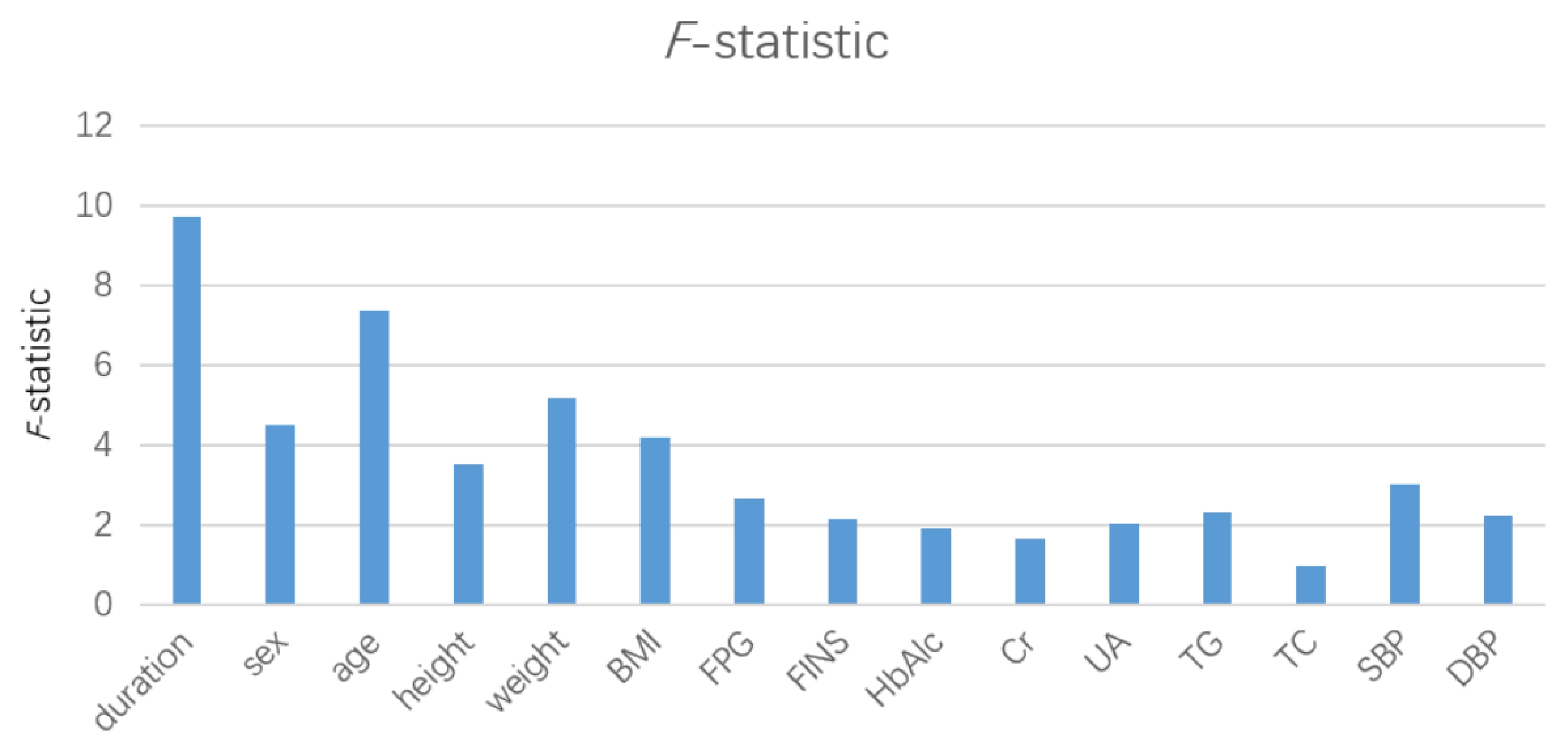
Figure 2. F-statistic in the multivariate linear regression model.
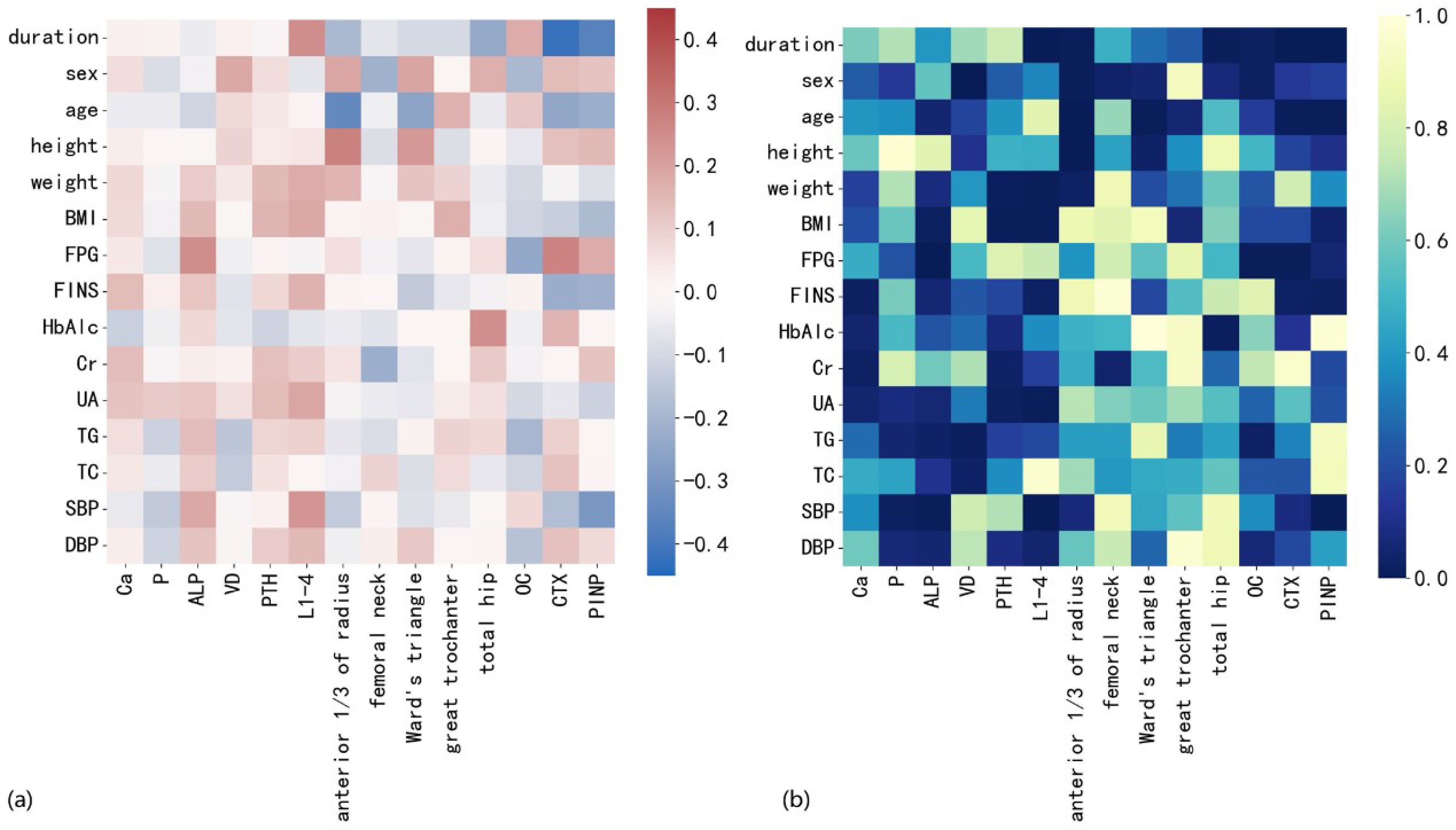
Figure 3. (a) Thermodynamic diagram of multiple linear regression equation coefficient (red represents positive correlation, blue represents negative correlation, and the darker the color, the larger the absolute value of the coefficient); (b) p value thermodynamic diagram of bone metabolism index and other data (the darker the color, the smaller the p value).
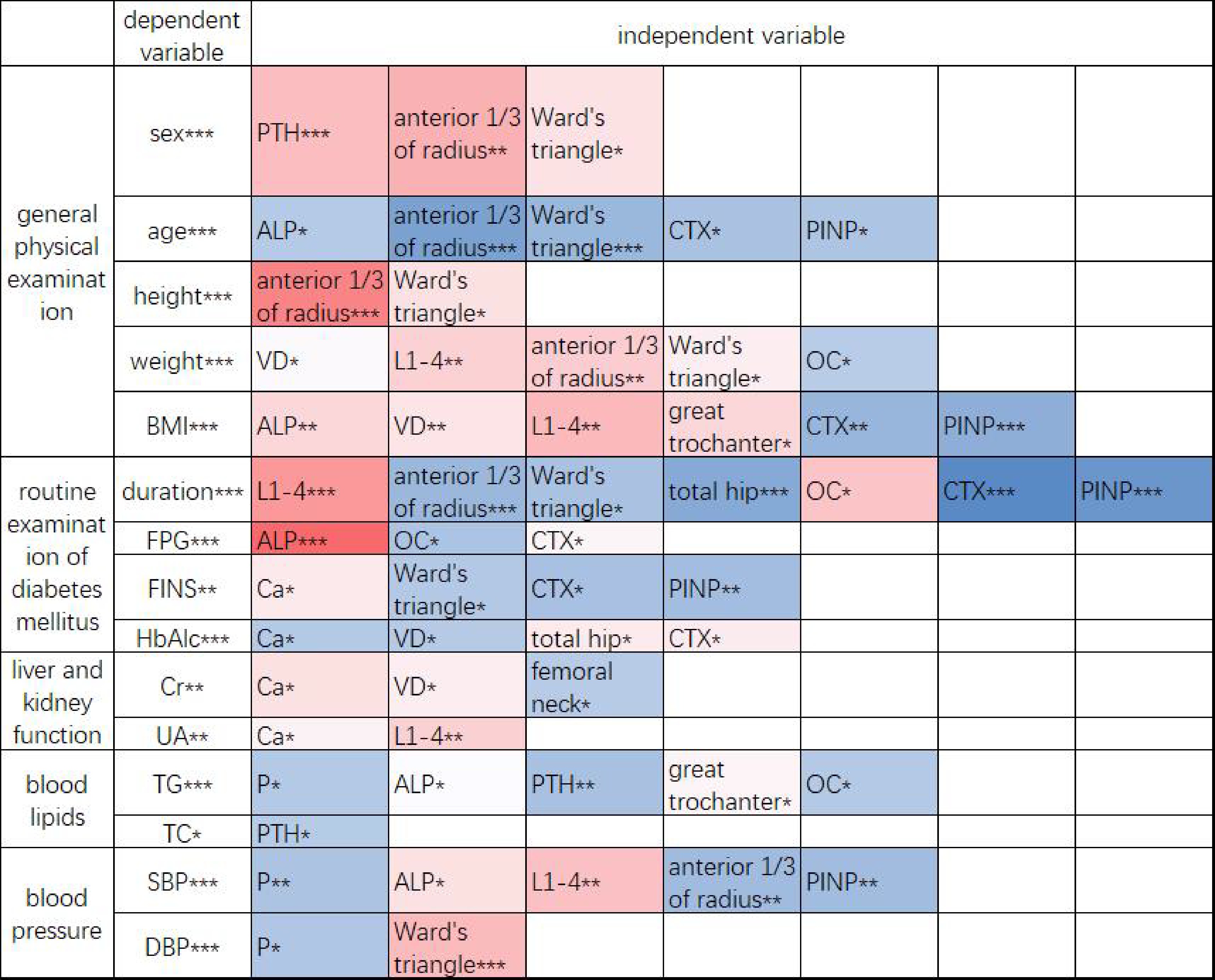
Figure 4. Thermodynamic diagram of the final equation coefficient of stepwise multiple linear regression. Red represents a positive correlation, and blue represents a negative correlation. The darker the color is, the larger the absolute value of the coefficient. *: p<0.05,**: p<0.01,***: p<0.001.
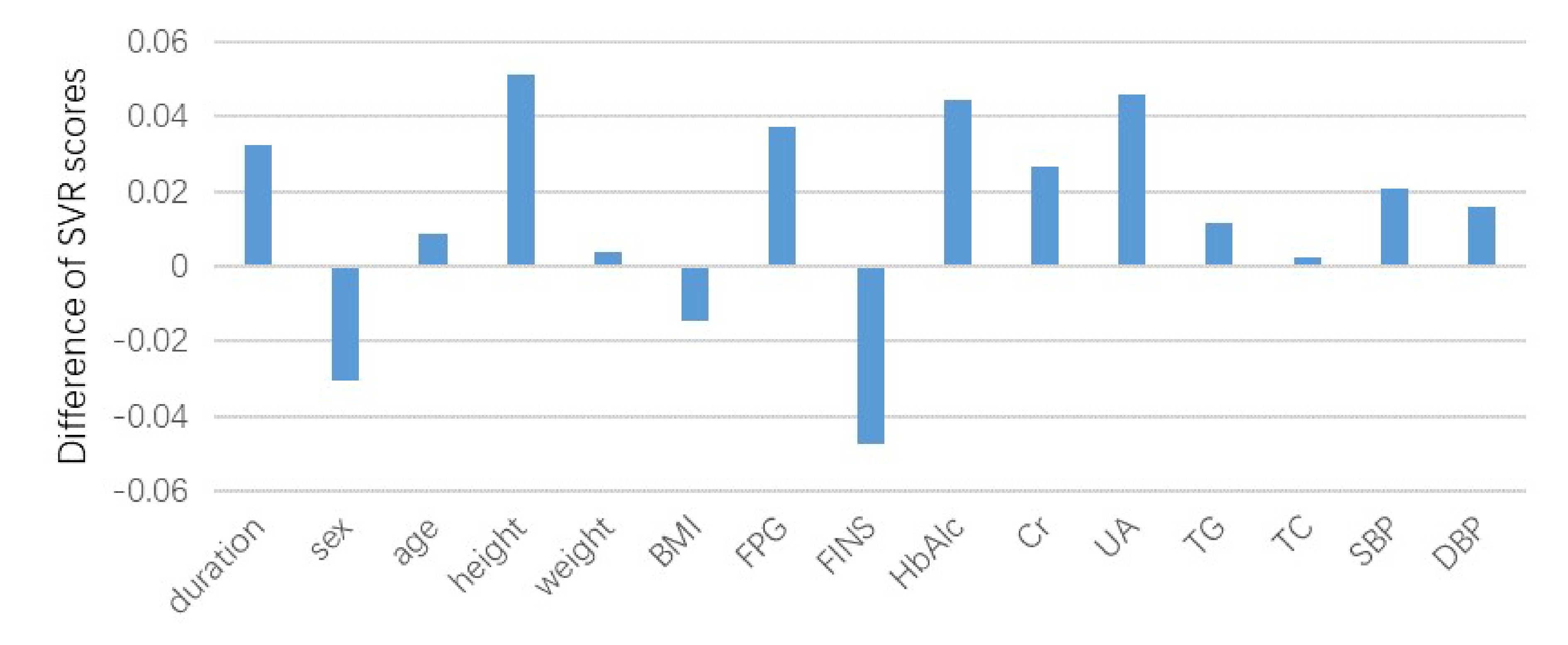
Figure 5. Differences in support vector regression model scores before and after screening.
| [1] |
Gregg E W, Li Y, Wang J, et al. Changes in diabetes-related complications in the United States, 1990–2010. The New England Journal of Medicine, 2014, 370 (16): 1514–1523. doi: 10.1056/NEJMoa1310799
|
| [2] |
King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. British Journal of Clinical Pharmacology, 1999, 48 (5): 643–648. doi: 10.1046/j.1365-2125.1999.00092.x
|
| [3] |
Sharma U, Pal D, Prasad R. Alkaline phosphatase: an overview. Indian Journal of Clinical Biochemistry, 2014, 29 (3): 269–278. doi: 10.1007/s12291-013-0408-y
|
| [4] |
Sabarudin A, Sakti S P, Aulanni’am, et al. Recent advances in nephropathy biomarker detections using paper-based analytical devices. Analytical Sciences, 2022, 38 (1): 39–54. doi: 10.2116/analsci.21SAR10
|
| [5] |
van Hoeven K H, Factor S M. The diabetic heart: clinical, experimental and pathological features. Acta Cardiologica, 1991, 46 (3): 329–339.
|
| [6] |
Wang J, Shu Y Q. Research progress in the pathogenesis of type 2 diabetic osteoporosis. Clinical Journal of Traditional Chinese Medicine, 2012, 24 (2): 183–184. (in Chinese) doi: 10.16448/j.cjtcm.2012.02.037
|
| [7] |
Sheu A, Greenfield J R, White C P, et al. Assessment and treatment of osteoporosis and fractures in type 2 diabetes. Trends in Endocrinology & Metabolism, 2022, 33 (5): 333–344. doi: 10.1016/j.tem.2022.02.006
|
| [8] |
Cai G Y, Ge X L, Wei L, et al. Observation of level of bone gla protein in serum. Chinese Journal of Osteoporosis, 1999, 5 (2): 29–32.(in Chinese)
|
| [9] |
Takashi Y, Kawanami D. The role of bone-derived hormones in glucose metabolism, diabetic kidney disease, and cardiovascular disorders. International Journal of Molecular Sciences, 2022, 23 (4): 2376. doi: 10.3390/ijms23042376
|
| [10] |
Krege J H, Lane N E, Harris J M, et al. PINP as a biological response marker during teriparatide treatment for osteoporosis. Osteoporosis International, 2014, 25 (9): 2159–2171. doi: 10.1007/s00198-014-2646-0
|
| [11] |
Delmas P D. Biochemical markers of bone turnover in Paget’s disease of bone. Journal of Bone and Mineral Research, 1999, 14: 66–69. doi: 10.1002/jbmr.5650140213
|
| [12] |
Mei C L, Wang N. Modern Regression Analysis Method (Chinese Edition). Beijing: Science Press, 2012 .
|
| [13] |
Wang J, Wang F, Liu Y, et al. Multiple linear regression and artificial neural network to predict blood glucose in overweight patients. Experimental and Clinical Endocrinology & Diabetes, 2016, 124 (1): 34–38. doi: 10.1055/s-0035-1565175
|
| [14] |
García-Martín A, Reyes-García R, García-Castro J M, et al. Role of serum FSH measurement on bone resorption in postmenopausal women. Endocrine, 2012, 41: 302–308. doi: 10.1007/s12020-011-9541-7
|
| [15] |
Cabrera C D, Henríquez M S, Traba M L, et al. Biochemical markers of bone formation in the study of postmenopausal osteoporosis. Osteoporosis International, 1998, 8 (2): 147–151. doi: 10.1007/BF02672511
|
| [16] |
Shan P F, Wu X P, Zhang H, et al. Bone mineral density and its relationship with body mass index in postmenopausal women with type 2 diabetes mellitus in mainland China. Journal of Bone and Mineral Metabolism, 2009, 27 (2): 190–197. doi: 10.1007/s00774-008-0023-9
|
| [17] |
Im J A, Yu B P, Jeon J Y, et al. Relationship between osteocalcin and glucose metabolism in postmenopausal women. Clinica Chimica Acta, 2008, 396 (1/2): 66–69. doi: 10.1016/j.cca.2008.07.001
|
| [18] |
Wei J, Karsenty G. An overview of the metabolic functions of osteocalcin. Current Osteoporosis Reports, 2015, 13 (3): 180–185. doi: 10.1007/s11914-015-0267-y
|
| [19] |
Rossini M, Gatti D, Zamberlan N, et al. Long-term effects of a treatment course with oral alendronate of postmenopausal osteoporosis. Journal of Bone and Mineral Research, 1994, 9 (11): 1833–1837. doi: 10.1002/jbmr.5650091121
|
| [20] |
Conte C, Epstein S, Napoli N. Insulin resistance and bone: a biological partnership. Acta Diabetologica, 2018, 55 (4): 305–314. doi: 10.1007/s00592-018-1101-7
|
| [21] |
Masaki H, Miki T. Bone and calcium metabolism in elderly women. Clinical Calcium, 2011, 21 (9): 1361–1367.
|
| [22] |
Keizman D, Ish-Shalom M, Berliner S, et al. Low uric acid levels in serum of patients with ALS: further evidence for oxidative stress? Journal of the Neurological Sciences, 2009, 285 (1/2): 95–99. doi: 10.1016/j.jns.2009.06.002
|
| [23] |
Ahn S H, Lee S H, Kim B J, et al. Higher serum uric acid is associated with higher bone mass, lower bone turnover, and lower prevalence of vertebral fracture in healthy postmenopausal women. Osteoporosis International, 2013, 24 (12): 2961–2970. doi: 10.1007/s00198-013-2377-7
|
| [24] |
Cui R, Zhou L, Li Z, et al. Assessment risk of osteoporosis in Chinese people: relationship among body mass index, serum lipid profiles, blood glucose, and bone mineral density. Clinical Interventions in Aging, 2016, 11: 887–895. doi: 10.2147/CIA.S103845
|
| [25] |
Ha J, Jo K, Lim D J, et al. Parathyroid hormone and vitamin D are associated with the risk of metabolic obesity in a middle-aged and older Korean population with preserved renal function: A cross-sectional study. PLoS ONE, 2017, 12 (4): e0175132. doi: 10.1371/journal.pone.0175132
|
| [26] |
Tintut Y, Parhami F, Tsingotjidou A, et al. 8-Isoprostaglandin E2 enhances receptor-activated NFκB ligand (RANKL)-dependent osteoclastic potential of marrow hematopoietic precursors via the cAMP pathway. The Journal of Biological Chemistry, 2002, 277 (16): 14221–14226. doi: 10.1074/jbc.M111551200
|
| [27] |
Go J H, Song Y M, Park J H, et al. Association between serum cholesterol level and bone mineral density at lumbar spine and femur neck in postmenopausal Korean women. Korean Journal of Family Medicine, 2012, 33 (3): 166–173. doi: 10.4082/kjfm.2012.33.3.166
|
| [28] |
He L, Huang L. Correlation between hypertension and primary osteoporosis. Modern Chinese Clinical Medicine, 2008, 15 (2): 1–3. (in Chinese)
|

ISSN 0253-2778
CN 34-1054/N
Copyright © Editorial Office of JUSTC, All Rights Reserved. 皖ICP备05002528号
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: